
Depression is frequently misunderstood as simply feeling “very sad.” In reality, chronic depression—clinically recognized as Major Depressive Disorder (MDD) or Persistent Depressive Disorder (Dysthymia)—is a complex neurobiological condition that impacts every facet of a person’s existence. It is not a choice, a character flaw, or a state of mind that someone can simply “snap out of.”
Modern psychiatry and neuroscience have advanced our understanding far beyond the simplistic “chemical imbalance” theory. While neurotransmitters like serotonin and dopamine are certainly involved, current research points to a broader systemic dysfunction within the brain’s circuitry, structure, and ability to adapt (neuroplasticity). This “brain storm” translates into specific, observable psychiatric and behavioral traits.
Understanding these traits is crucial for recognizing the illness, validating the experience of those living with it, and tailoring effective treatments. Here, we explore the top 10 most common psychiatric traits found in depressed people, bridging the neurological underpinnings with their behavioral manifestations.
1. Anhedonia: The Lost Capacity for Pleasure
Anhedonia is one of the two core diagnostic criteria for MDD, but it is often deeply overlooked. It isn’t just about feeling “down”; it is the core inability to experience joy, interest, or satisfaction from activities that were previously pleasurable. Imagine your favorite food tasting like ash, or your favorite hobby feeling like a chore.
The Neurology: Anhedonia points to dysfunction in the brain’s reward system, particularly the Nucleus Accumbens and its connections to the prefrontal cortex. Depressed individuals show reduced response to pleasant stimuli in these areas, coupled with lower levels of dopamine signaling, the neurotransmitter responsible for anticipating and experiencing reward. The “engine” for joy is simply failing to fire.
The Behavioral Manifestation: A person with anhedonia might stop engaging in hobbies, detach from social groups, show no enthusiasm for milestones, and lose libido. This trait creates a powerful feedback loop of isolation, as the individual ceases the activities that might otherwise boost their mood.
2. Psychomotor Retardation or Agitation: The Mind-Body Slump
Mental pain frequently manifests physically. For many, depression is a state of “unbearable slowness.” Speech may be slowed, movements become laborious, and even a simple task like brushing teeth feels as if one is moving through water. Conversely, others experience “agitation”—fidgeting, pacing, and restlessness that stems from an internal sense of tension.
The Neurology: This trait is linked to metabolic abnormalities and structural changes in key brain areas. Psychomotor retardation is often associated with dysregulation in the Basal Ganglia (critical for motor control) and reduced activity in the motor cortex. It reflects a profound decoupling between the will to move and the body’s execution.
The Behavioral Manifestation: Observers may notice that a depressed person takes a long time to answer a question or speaks in a monotonic, hushed tone. The agitation, while outwardly energetic, is unproductive, driven by anxiety rather than energy. This trait directly contributes to the overwhelming “lead-heavy” exhaustion so common in the condition.
3. Chronic Fatigue and Energy Depletion
Linked closely to psychomotor symptoms is the relentless fatigue that defies rest. It is a profound, systemic lack of energy that persists despite adequate sleep. For those with chronic depression, this fatigue is not laziness; it is an all-encompassing neurological state.
The Neurology: Several pathways are involved. The hypothalamic-pituitary-adrenal (HPA) axis, which regulates stress responses and cortisol, is often chronically hyperactive in depressed patients, leading to eventual adrenal exhaustion and metabolic breakdown. Furthermore, there are indications of mitochondrial dysfunction (the “power plants” of our cells failing to produce energy efficiently) and an overall inflammatory state that mimics the symptoms of acute illness (the “flu-like” feeling).
The Behavioral Manifestation: This fatigue is the “wall” that stops life. It leads to severe difficulties in getting out of bed, managing basic hygiene, going to work, or making decisions. The energy required to simply “be” consumes everything else, forcing the brain and body into a conservation mode that resembles hibernation.
4. Cognitive Dysfunction and “Brain Fog”
Depression attacks the mind’s operations, not just its feelings. People with chronic depression often struggle with severe difficulties in concentration, making decisions, or finishing tasks. Simple multi-step problems become insurmountable, and a pervasive, opaque “fog” blankets their thoughts.
The Neurology: This trait maps precisely to functional and structural changes in the Prefrontal Cortex (PFC), the brain’s center for executive function, logic, and working memory. Research frequently finds reduced activation and even decreased grey matter volume in this critical area, meaning the part of the brain responsible for focusing and planning is running with limited resources.
The Behavioral Manifestation: A common complaint is an inability to read a page of a book and remember what was just read, leading many to feel they are losing their intelligence. The profound indecisiveness (e.g., spending 20 minutes unable to decide what to eat) is a direct consequence of the PFC struggling to process and prioritize competing information.
5. Persistent Rumination and Cognitive Rigidity
Ruminating is the process of obsessively spinning positive or negative thoughts without reaching a resolution. Depressed individuals get “stuck” in loops of past failures, perceived flaws, and future worries. This is coupled with “rigidity”—the profound difficulty in viewing a situation from a different perspective, reinforcing a hopeless narrative.
The Neurology: Rumination is visible on brain scans as a hyper-connected, overactive Default Mode Network (DMN). This is the circuit that becomes active when we are reflecting on ourselves. When the DMN fails to “switch off” as the brain attempts to focus on external tasks, it forces the mind to constantly turn inward, re-playing its self-critical playlist.
The Behavioral Manifestation: The person may appear distracted, as their mind is occupied by internal static. This constant internal critique fuels feelings of guilt and worthlessness and makes problem-solving impossible, as they cannot access the “flexibility” required to see potential solutions.
6. Circadian Dysregulation (Sleep Disturbances)
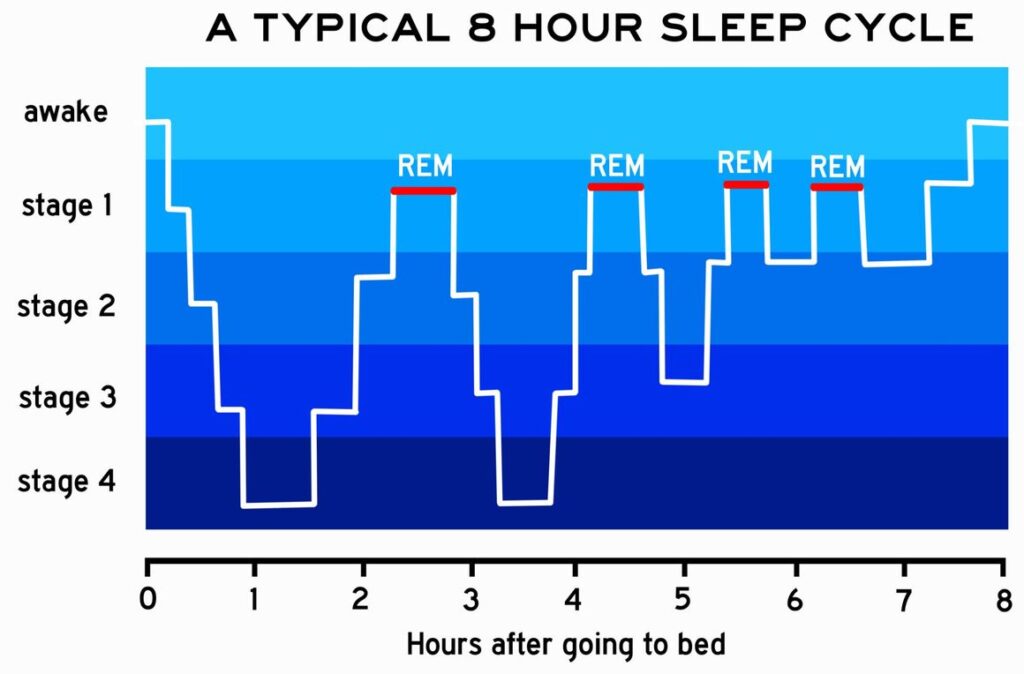
Sleep and depression are deeply, biologically intertwined. The vast majority of depressed people experience sleep disturbances, most commonly insomnia (difficulty falling asleep or staying asleep, or particularly, terminal insomnia, waking up very early). However, some experience hypersomnia (excessive sleeping, often exceeding 12 hours).
The Neurology: Depression severely disrupts the brain’s master clock, the Suprachiasmatic Nucleus (SCN), which governs our circadian rhythms. Depressed patients often exhibit flattened cortisol rhythms (lacking the normal morning spike that wakes us) and dysregulated melatonin production. Furthermore, they show abnormalities in REM sleep (dream sleep), often entering it too quickly and extensively, which can be exhausting in itself.
The Behavioral Manifestation: Poor sleep creates a compounding catastrophe, severely exacerbating fatigue and cognitive fog. For many, a powerful diagnostic clue is diurnal variation: symptoms are devastatingly worse in the early morning (driven by the low energy and cortisol lows) and slightly lift in the evening.
7. Social Isolation and Withdrawal
Isolation is both a symptom and a magnifier of depression. Depressed individuals often feel an agonizing desire to disappear. They avoid social contact, ignore texts, cancel plans, and retreat from relationships, creating a profound, painful “cocoon.”
The Neurology: Isolation is a behavioral response driven by multiple brain systems. Chronic activation of the Amygdala (fear center) makes social interactions feel threatening rather than rewarding. This combines with the lack of dopamine (anhedonia), making the perceived energy cost of socializing feel monumental, with no expected pleasure (reward) to justify it.
The Behavioral Manifestation: This trait is often the most visible warning sign. A previously social person stops appearing at gatherings or interacting online. This profound loneliness, paradoxically fueled by their own avoidance, strengthens the narrative that they are a “burden” or that “no one cares,” intensifying the depression.
8. Negative Cognitive Bias and Distorted Memory
A depressed brain does not see the world as it is; it sees it through a powerful filter of hopelessness. When presented with ambiguous information, it will always interpret it negatively. Furthermore, it exhibits a striking memory bias: it vividly and readily recalls every past failure or trauma while struggling to access memories of success or happiness.
The Neurology: This is a problem of communication between the Amygdala (emotion) and the Hippocampus (memory). The overactive amygdala essentially “tags” stressful or painful memories with massive emotional importance, ensuring they are easily retrieved, while suppressing the consolidation of positive experiences.
The Behavioral Manifestation: This distortion fuels the profound feelings of worthlessness (“I always fail”) and hopelessness (“It has always been this way and always will be”). Therapy—particularly CBT—is designed specifically to address this bias by teaching people to recognize and challenge these distorted thought patterns.
9. Learned Helplessness and Avolition
Avolition is a psychological term for a severe lack of initiative or motivation to start or complete any task. Closely related is “learned helplessness,” a belief system that forms when one perceives they have no control over negative events, leading to a state of resignation and inertia.
The Neurology: This trait is strongly linked to persistent dysregulation within the brain’s main Serotonin center, the Dorsal Raphe Nucleus. In states of chronic stress and depression, the brain essentially “adapts” to a perceived hostile, unpredictable environment by entering a passive survival mode. When control feels lost, motivation simply shuts down.
The Behavioral Manifestation: This is the force that paralyzes action. It prevents a person from taking proactive steps to help themselves (e.g., booking a therapy appointment, preparing healthy food), as they do not believe their efforts will make any difference. This can be interpreted by outsiders as apathy, but it is better understood as a breakdown of the neurological mechanisms that connect effort to outcome.
10. Somatic Symptoms and Unexplained Pain
Finally, chronic depression is frequently a disease that hurts physically. Patients commonly report chronic headaches, mysterious back or joint pain, and severe digestive issues (like Irritable Bowel Syndrome), all of which have no clear, direct physical cause.
The Neurology: Psychology has long recognized that emotional pain is processed using many of the same neural circuits as physical pain. The Anterior Cingulate Cortex (ACC) and the Insula are hyper-sensitive in depressed individuals. This means the sensory input from the body is interpreted differently, amplifying sensations and lowering the brain’s pain tolerance threshold. Depression essentially “turns up the volume” on any mild physical discomfort.
The Behavioral Manifestation: These chronic physical aches and digestive issues contribute significantly to the perceived illness and can lead to over-utilization of general medical services, delaying correct psychiatric diagnosis and treatment.
Conclusion: Why These Traits Matter in Modern Psychiatry
Understanding that chronic depression is a systemic state of the brain that manifests as these 10 distinct, observable traits has profoundly changed how psychiatrists approach treatment.
- Treatment Must Be Targeted: We no longer rely on a “one-size-fits-all” antidepressant (which typically focuses on Serotonin). For example, if a patient’s profile is dominated by Anhedonia (1) and Avolition (9), we might choose a medication that targets Dopamine and Norepinephrine. If their primary issue is Sleep Dysregulation (6), we prioritize circadian therapies.
- Psychotherapy is Neurological: When therapy helps a patient break a cycle of Rumination (5) or correct their Negative Memory Bias (8), they are not just “talking.” They are engaging in “top-down” neural reorganization, strengthening the Prefrontal Cortex (4) to exert control over the Amygdala (8), actively rewiring their own circuitry.
- Whole-Body Medicine is Essential: We must acknowledge the Somatic (10), Fatigue (3), and Inflammatory components. Effective treatment often moves beyond psychiatry to include metabolic health, nutrition, and anti-inflammatory strategies.
Recognizing these traits validates the devastating physical, behavioral, and mental reality of chronic depression. For those living with it, and those treating it, the realization that these symptoms have specific neurobiological footprints can provide clarity, reduced guilt, and—most importantly—a pathway to targeted, effective healing.



Leave a Reply