For decades, modern medicine viewed sleep disruption as nothing more than a secondary footnote. If you struggled with severe anxiety, clinical depression, or chronic stress, a restless night was simply dismissed as a predictable side effect—the natural fallout of a troubled mind.
But a quiet revolution at the intersection of neuroscience, cognitive psychology, and clinical psychiatry has completely upended this old paradigm.
We now know that the relationship between your brain and the pillow is not a one-way street. It is a complex, hyper-dynamic, bidirectional loop. Your sleep architecture does not merely reflect your psychological state; it actively constructs, regulates, and alters your mental health every single night.
To ignore the mechanics of sleep is to ignore the foundation of neural recovery itself. Understanding how sleep, psychology, and psychiatry converge offers an incredibly powerful framework for optimizing your cognitive longevity, rebuilding emotional resilience, and taking proactive control of your mind.
The Architecture of the Nocturnal Mind: A Psychological Overhaul
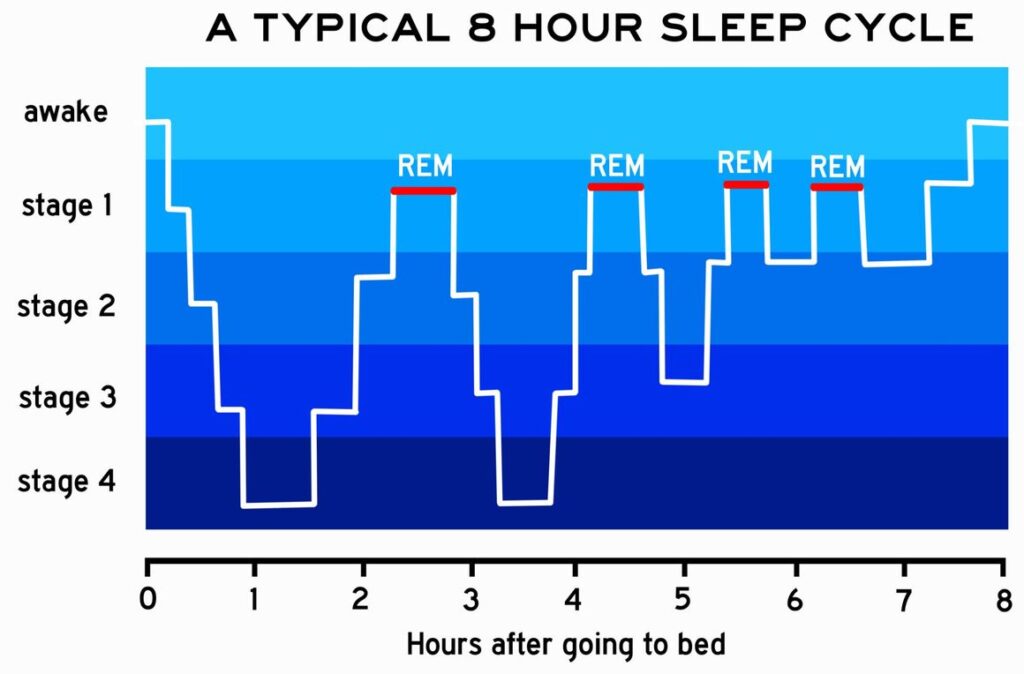
To understand why a lack of sleep fractures our psychological well-being, we have to look closely at what the brain is actually doing while we are unconscious. Sleep is far from a passive state of biological dormancy. It is an incredibly active, highly coordinated series of stages, each designed to perform specific cognitive maintenance.
The human brain relies on two primary types of sleep to maintain psychological homeostasis (balance): Deep Sleep (Slow-Wave Sleep) and REM (Rapid Eye Movement) Sleep.
The Emotional Therapy of REM Sleep
During the day, your brain absorbs countless stimuli, emotional micro-traumas, and complex social interactions. If these experiences remained raw and unparsed, your nervous system would quickly collapse under the weight of chronic hyperarousal.
Enter REM sleep. Often referred to by neuroscientists as a form of “overnight therapy,” REM sleep is the only time your brain completely shuts off the release of noradrenaline (a major stress chemical related to adrenaline). While your brain is dreaming, it replays the emotional memories of your day in a completely calm, neurochemically safe environment.
This process strips the painful, visceral “sting” away from your memories, leaving behind the valuable information while discarding the stressful emotional reaction. When you miss out on high-quality REM sleep, you wake up with your emotional reactivity fully intact. The brain remains trapped in a state of high alarm, interpreting neutral daily interactions as active threats.
Deep Sleep and Executive Function
While REM sleep handles your emotional processing, Deep Sleep handles the structural maintenance of your physical brain. During slow-wave sleep, the brain’s glymphatic system (the brain’s internal waste clearance system) opens up, washing away metabolic waste products like beta-amyloid proteins that accumulate during waking hours.
Simultaneously, the brain engages in synaptic pruning—a vital psychological process where weak or unnecessary neural connections are cleared out, and critical connections are reinforced. Without this nightly optimization, your prefrontal cortex—the seat of impulse control, logical reasoning, and emotional regulation—suffers from severe executive dysfunction the following day.
The Psychiatric Crossroads: Disrupted Cycles and Clinical Disorders
Where psychology looks at the behavioral and emotional patterns of sleep, psychiatry examines the underlying neurobiology, brain chemistry, and clinical pathologies. In psychiatric science, sleep architecture is often the first domino to fall before a major mental health crisis.
| Psychiatric Condition | Sleep Architecture Abnormality | Clinical Consequence on Patient |
| Major Depressive Disorder (MDD) | Premature REM onset; reduction in deep slow-wave sleep. | Severe morning fatigue, flattened affect, and emotional dysregulation. |
| Generalized Anxiety Disorder (GAD) | Prolonged sleep latency (takes over 30 mins to sleep); sleep fragmentation. | Hypervigilant nervous system, elevated baseline cortisol levels. |
| Bipolar Disorder | Sudden, drastic decrease in the biological need for sleep. | Often serves as the primary behavioral trigger for a manic episode. |
| ADHD | Circadian rhythm phase delay (shifted biological clock). | Compounded executive dysfunction, daytime sleepiness, and impulsivity. |
The Cortisol-Insomnia Feedback Loop
In psychiatry, the “bidirectional trap” is best illustrated by the relationship between chronic insomnia and anxiety disorders. When an individual experiences prolonged psychological stress, the body’s hypothalamic-pituitary-adrenal (HPA) axis becomes chronically overactive. This causes a continuous, systemic flooding of cortisol and adrenaline into the bloodstream.
This chemical hyperarousal makes falling asleep biologically difficult. As sleep deprivation sets in, the amygdala (the brain’s emotional fire alarm) becomes up to 60% more reactive to negative stimuli. The weakened prefrontal cortex can no longer regulate or calm the amygdala down, leading to increased daytime anxiety, which further fuels nocturnal hyperarousal. Breaking this psychiatric loop requires treating the brain chemistry and the behavioral sleep cycle simultaneously.
The Silent Menace: Sleep Apnea and Misdiagnosed Psychiatric Symptoms
One of the most critical challenges in modern psychiatry is the overlap between structural sleep disorders and psychiatric symptoms. The most notable culprit is Obstructive Sleep Apnea (OSA)—a condition where the airway repeatedly collapses during the night, starving the brain of oxygen and causing micro-awakenings that tear sleep architecture to shreds.
Because the brain is repeatedly starved of oxygen, individuals with untreated sleep apnea frequently present with symptoms that perfectly mimic clinical depression and severe generalized anxiety:
- Chronic morning brain fog and anhedonia (inability to feel pleasure)
- Extreme emotional volatility and irritability
- Panic attacks upon waking (caused by sudden drops in blood oxygen levels triggering a primal suffocation response)
When a patient seeks psychiatric care for treatment-resistant depression, a thorough assessment often reveals that the root cause isn’t a baseline chemical imbalance, but rather a hidden, nocturnal respiratory issue. Treating the physical sleep disorder frequently resolves the psychological symptoms entirely, illustrating just how profoundly our mental wellness depends on physical sleep integrity.
Behavioral Psychiatry in Action: Moving Beyond the Sleeping Pill
For decades, the standard response to psychiatric sleep issues was a prescription for sedatives or hypnotic sleep medications. While these interventions can offer short-term relief during acute crises, clinical data has conclusively demonstrated that pharmaceutical sedation is not the same as natural, restorative sleep. Many traditional sleep medications actually suppress REM and deep sleep stages, leaving the patient structurally sleep-deprived despite being unconscious for eight hours.
Because of this, modern psychiatry and cognitive psychology have shifted their gold-standard treatment to a behavioral intervention: CBT-I (Cognitive Behavioral Therapy for Insomnia).
How CBT-I Rewires the Brain
CBT-I is an evidence-based psychological framework designed to dismantle the toxic mental associations that form during chronic insomnia. When a person struggles to sleep, they begin to associate their bed with frustration, fear, and panic. CBT-I uses specific behavioral conditioning techniques to break this link:
- Stimulus Control: Re-anchoring the bed as a place of pure rest. If you are not asleep within twenty minutes, you must physically leave the bed. This prevents the brain from reinforcing the neural pathway that connects the bedroom with stressful wakefulness.
- Sleep Restriction: Temporarily limiting the time spent in bed to closely match the patient’s actual sleep time. This builds up an intense biological “sleep drive,” training the brain to consolidate sleep into a solid, unbroken block rather than a fragmented, shallow experience.
- Cognitive Restructuring: Systematically challenging the catastrophic thought patterns (“If I don’t sleep tonight, my career will fall apart tomorrow”) that trigger cortisol spikes right before midnight.
A Protocol for Cognitive Longevity and Emotional Resilience
Optimizing your mental health through the lens of sleep science requires a deliberate, daily commitment to your biological rhythms. Your circadian rhythm runs on a roughly 24-hour cycle, meaning the choices you make at 8:00 AM directly dictate your brain’s capacity for deep recovery at 10:00 PM.
Phase 1: The Morning Anchor (Cortisol & Light)
- View Immediate Sunlight: View natural, unfiltered sunlight within 30 minutes of waking up for at least 10 to 15 minutes. This triggers an immediate, healthy spike in morning cortisol (setting your internal waking clock) and stops the production of lingering melatonin.
- Delay Caffeine Intake: Wait 90 to 120 minutes after waking to consume caffeine. This allows your brain to naturally clear out adenosine (the chemical built up during the day that causes sleepiness), preventing a severe afternoon crash that disrupts evening relaxation.
Phase 2: The Evening Transition (Melatonin Protection)
- Eliminate Blue Light Exposure: Turn off overhead lights and eliminate bright blue-light exposure from screens at least two hours before bed. Blue light hits specific receptors in your eyes that trick the brain into thinking it is noon, instantly delaying your body’s natural melatonin release.
- Cool the Body’s Core Temperature: Your brain requires your core body temperature to drop by about two degrees Fahrenheit to transition into deep sleep. Taking a hot shower or bath 90 minutes before bed brings blood flow to the surface of your skin, releasing heat and forcing your core temperature to plummet rapidly once you step out.
Conclusion: Honoring the Nocturnal Edge
True mental performance, psychological well-being, and long-term cognitive health cannot be achieved through sheer force of will, nor can they be sustained when your sleep architecture is fractured. Sleep is the ultimate biological optimizer—it is a non-negotiable, natural defense mechanism that shields us against the challenges of daily life.
By treating sleep optimization not as an afterthought, but as an essential, proactive tool of behavioral psychiatry, you unlock a profound mental health advantage. Making conscious, scientifically backed lifestyle choices allows you to wake up with an emotionally balanced, structurally fortified mind.
To explore more comprehensive, expert-led guides designed to build a lifelong cognitive edge, check out the mental wellness and brain health insights over at yourise.me, where leading-edge tech and practical neuroscience converge to help you optimize your daily life. Stop treating sleep as a luxury; treat it as the very foundation of your psychological strength.



Leave a Reply